Concerns over the Seroxat Group Litigation - new blog
see -
http://the-uk-seroxat-litigation-chronicles.blogspot.com/
I’m taking time out from statistics and associated issues - as yet unpublished - to facilitate publishing information appertaining to the UK Seroxat Litigation which, having been in the public domain since it was preannounced in 2001/2, is going to court this year.
The information encompasses the UK Government Prescription Cost Analysis (PCA) statistics - although at the time of publication of my UK: SSRI / SNRI Antidepressant Statistical Politics Blog - I was unaware of one significant fact and therefore revelations were unintentional.
However, a few weeks after my blogs publication, on first sight of the Seroxat Group Litigation Order no: 68 it became glaringly obvious that inadvertently, the statistics – not me – undermine the Litigation.
Since becoming aware of and involved with the SSRI drug forums in 2001, I have spoken out - not against the litigation - but in concern for those involved and anyone taking SSRI, SNRI drugs, especially those choosing to or being swapped without consideration from Seroxat to other drugs in the class including Prozac, Lustral and Efexor.
The statistics are, unfortunately, not the only jeopardy to the frail legal case being successful - Seroxat has a certain notoriety for being “the worst drug” in the class - but is that notoriety well-substantiated or solely due to outside influences? Do the experts agree?
Have the UK population been let down by the government, medicines authorities and the media?
The following will possibly adversely impact on the few hundred people who have not been culled from the originally quoted 10.000 prospective litigants ...... but the full ramifications of not speaking out will possibly impact on thousands or even millions.
This blog will hopefully extricate the distinct facts, clarify, assemble and publicise each in context - to let the readers decide for them selves.
I have no conflicting interests.
Sunday, 31 January 2010
Saturday, 30 January 2010
FETAL ANTI-CONVULSANT LITIGATION: WILL LSC FUNDING LIMITATIONS LEAD TO THE COLLAPSE OF YET ANOTHER PHARMACEUTICAL GROUP ACTION
In the case of Multiple Claimants v Sanofi-Synthelabo [2007] EWHC 1860 (QB)1 (commonly known as the fetal anti-convulsant (“FAC”) litigation) the claimants failed in their application for an order for the trial of certain dispositive preliminary issues on the basis of assumed facts. With Legal Services Commission ("LSC") funding having been granted on the basis that the matter would proceed by way of a trial on the "preliminary issue on defect", it now remains to be seen whether this litigation will join the roll-call of high-profile pharmaceutical product liability actions which have met an early demise due to the cessation of public funding.
Background
The claimants are children whose mothers had, during their pregnancy, taken an anti-epileptic drug called sodium valproate, manufactured by the defendants and marketed under the name Epilim. The claimants allege that Epilim is a defective product within the meaning of the Consumer Protection Act 1987 (“CPA”). This provides that liability will attach if the safety of a product is not such as persons are generally entitled to expect. The claimants brought their actions pursuant to the Congenital Disabilities (Civil Liability) Act 1976 (“CDCLA”), which governs claims for pre-natal injuries. The claimants’ contention is that they were born disabled as a result of an “occurrence” within the meaning of s 1(2)(b) of the CDCLA and
s 6(3) of the CPA (which deals with how the CDCLA is to be given effect in relation to
1 The Defendant is incorrectly described as Sanifo-Synthelabo in the official judgment heading. liability for defective products). The occurrence was said to be “the transplacental spread of sodium valproate or its metabolites to the embryo/fetus, which then affected the embryonic and fetal development and organogenesis”.
The claimants allege that the defect that caused the occurrence was the teratogenic capacity of sodium valproate. Their primary case is that the information supplied with Epilim to a user is not a relevant circumstance when assessing the legitimate expectation of safety of persons generally for the purposes of the CPA. They also submit that the information provided by the defendants was inadequate.
The defendants say that the current state of scientific knowledge does not permit any of the anti-epileptic drugs currently on the market to be deemed free of teratogenic potential. They deny that a product such as Epilim is defective within the meaning of the CPA where, by its very nature, its use carries a potential risk of adverse events and those risks are generally known to treating practitioners and/or specifically warned about by the marketing authorisation holder. They also argue that the claimants’ case is bad in law as the CPA cannot be construed to require a court to disregard the essential factual context of the guidance or warnings provided as to adverse events or harmful characteristics of the product.
The Funding of the Case
The claimants had originally been granted funding by the LSC to pursue to trial their cases as to liability and generic causation, subject to an annual affordability review. In August 2006 the LSC notified the claimants of a decision that effectively brought the funding to an end. Judicial review proceedings were subsequently instituted and the LSC’s decision to withdraw the funding was quashed. The LSC then agreed to provide some limited funding.
A witness statement of the director of the LSC's Special Cases Unit, which is responsible for managing funding for complex or high cost civil cases, was put before Mr Justice Smith at the hearing of the claimants' application. In the statement, he referred to some of the matters identified at Rule 1.1(2) of the Civil Procedure Rules as aspects of dealing with a case justly. He stated: “Ensuring that high cost civil cases are subject to appropriate financial controls requires case managers to ensure funded cases comply with the spirit of the Woolf reforms, in particular the overriding objectives of saving expense and dealing with the case in ways which are proportionate given the amount of money involved, the importance of the case and the complexity of the issues.”
It is stated at the outset of the Civil Procedure Rules that they have the “overriding objective of enabling the court to deal with cases justly.” Mr Justice Smith noted that the director made no mention in his statement of the other matters referred to in CPR 1.1(2) such as ensuring that the parties are on an equal footing (CPR
DISPUTE RESOLUTION
OCTOBER 2007
THE FETAL ANTI-CONVULSANT LITIGATION: WILL LSC FUNDING LIMITATIONS LEAD TO THE COLLAPSE OF YET ANOTHER PHARMACEUTICAL GROUP ACTION?
1.1(2)(a)), dealing with the case in ways which are proportionate to the financial position of each party (CPR 1.1(2)(c)(iv)), and ensuring that the case is dealt with expeditiously and fairly (CPR 1.1(2)(d)). According to the director’s statement, the LSC appeared to have elevated some of the various elements that the CPR identify as contributing to the overriding objective into distinct overriding objectives in their own right. Mr Justice Smith said he did not consider this to be helpful as the court has to seek to give effect to the overriding objective as a whole.
The director explained that following the decision in the judicial review proceedings, the LSC’s Funding Review Committee (“FRC”) concluded that the case “had sufficient merits to meet the merits test contained within the Funding Code as long as the case proceeded on the basis that the preliminary issue on defect, which was alone capable of derailing the litigation, was decided first…” If the case could not proceed by way of a trial on a preliminary issue then the case would be sent back to the FRC for review.
The Court’s Findings
The claimants therefore applied to have certain preliminary issues determined first. At the hearing, the claimants’ counsel expressed the opinion that unless the court acceded to the views of the LSC as to how this litigation should proceed, it was likely that funding would be discontinued. However, Mr Justice Smith thought this submission went further than the director’s evidence.
Assumptions
Mr Justice Smith firstly considered the assumptions upon which the claimants proposed that the preliminary issues be tried. He noted that particularly in complex cases, it was necessary that the assumptions be precise and unambiguous, as much of the purpose of having preliminary issues would be lost if the assumptions had to be expanded and explained by complicated scientific and pharmacological evidence.
His Honour found that the assumptions in the instant case did not, and however drafted could not, provide a clear and precise factual basis for the determination of the issues. For example, one of the claimants’ assumptions was that Epilim “is unsafe for all pregnant women whose fetuses are exposed to it.” Yet, it was unclear what the description of “unsafe” meant. Nor was it clear what was the degree of risk and what potential damage and/or disabilities would be sufficient for the drug to be described this way. Whilst he accepted that it may be necessary to supplement assumptions with some limited evidence, the more that is required, the less attractive the proposal for preliminary issues becomes.
Preliminary Issues
Mr Justice Smith then considered the preliminary issues that the claimants proposed and found these to also be problematic. For example, one of the issues assumed there had been an "occurrence" when this was still in dispute. Another issue could not be satisfactorily decided without a firm factual and evidential basis. Mr Justice Smith therefore rejected the claimants’ application for an order for the trial of the questions as preliminary issues.
Comment
It remains to be seen whether the LSC will now pull the plug on the funding of the FAC litigation - an outcome that the claimants' counsel clearly thought was likely. Without public funding, this litigation will inevitably become the latest in a long list of group actions doomed to failure in recent years. The LSC currently funds major group actions out of a budget of £3m per annum, which potentially limits the scope of major new group litigation. Funding for group actions is under far greater control than ever before through the LSC’s Special Cases Unit and in a recent article Colin Stutt, the Head of Funding Policy at the LSC, noted that pharmaceutical actions remain “very problematic”2.
However, there may be some light at the end of the tunnel for claimants hoping to pursue pharmaceutical group actions in the future. In June this year a series of recommendations were made by the Civil Justice Council to the Lord Chancellor to improve access to justice through the development of improved funding structures.3 One of the recommendations was for the introduction of properly regulated contingency fees in multi party cases where no other form of funding is
2 C Stutt, “Who ate all the P.I.’s?” (2007) JPIL 81 at 82.
3 Civil Justice Council, “The Future Funding of Litigation – Alternative Funding Structures” June 2007. available. It may well be that contingency fees will become the mainstream funding alternative for pharmaceutical group actions in future, given the continued tightening of the LSC’s purse strings for such cases. However, the introduction of any such reforms is likely to come too late for the claimants in the FAC litigation.
If you would like any further information, please contact either of the following:
Simon Pearl
DDI: 020 7293 4041
E: spearl@dac.co.uk
Olya Melnitchouk
DDI: 020 7293 4506
E: omelnitchouk@dac.co.uk
This publication is not a substitute for detailed advice on specific transactions and problems and should not be taken as providing legal advice on any of the topics discussed.
name and company name.
http://www.dac.co.uk/documents/resources/newsletters/The_fetal_anti_convulsant_litigation_Dispute_Resolution_Wire
Background
The claimants are children whose mothers had, during their pregnancy, taken an anti-epileptic drug called sodium valproate, manufactured by the defendants and marketed under the name Epilim. The claimants allege that Epilim is a defective product within the meaning of the Consumer Protection Act 1987 (“CPA”). This provides that liability will attach if the safety of a product is not such as persons are generally entitled to expect. The claimants brought their actions pursuant to the Congenital Disabilities (Civil Liability) Act 1976 (“CDCLA”), which governs claims for pre-natal injuries. The claimants’ contention is that they were born disabled as a result of an “occurrence” within the meaning of s 1(2)(b) of the CDCLA and
s 6(3) of the CPA (which deals with how the CDCLA is to be given effect in relation to
1 The Defendant is incorrectly described as Sanifo-Synthelabo in the official judgment heading. liability for defective products). The occurrence was said to be “the transplacental spread of sodium valproate or its metabolites to the embryo/fetus, which then affected the embryonic and fetal development and organogenesis”.
The claimants allege that the defect that caused the occurrence was the teratogenic capacity of sodium valproate. Their primary case is that the information supplied with Epilim to a user is not a relevant circumstance when assessing the legitimate expectation of safety of persons generally for the purposes of the CPA. They also submit that the information provided by the defendants was inadequate.
The defendants say that the current state of scientific knowledge does not permit any of the anti-epileptic drugs currently on the market to be deemed free of teratogenic potential. They deny that a product such as Epilim is defective within the meaning of the CPA where, by its very nature, its use carries a potential risk of adverse events and those risks are generally known to treating practitioners and/or specifically warned about by the marketing authorisation holder. They also argue that the claimants’ case is bad in law as the CPA cannot be construed to require a court to disregard the essential factual context of the guidance or warnings provided as to adverse events or harmful characteristics of the product.
The Funding of the Case
The claimants had originally been granted funding by the LSC to pursue to trial their cases as to liability and generic causation, subject to an annual affordability review. In August 2006 the LSC notified the claimants of a decision that effectively brought the funding to an end. Judicial review proceedings were subsequently instituted and the LSC’s decision to withdraw the funding was quashed. The LSC then agreed to provide some limited funding.
A witness statement of the director of the LSC's Special Cases Unit, which is responsible for managing funding for complex or high cost civil cases, was put before Mr Justice Smith at the hearing of the claimants' application. In the statement, he referred to some of the matters identified at Rule 1.1(2) of the Civil Procedure Rules as aspects of dealing with a case justly. He stated: “Ensuring that high cost civil cases are subject to appropriate financial controls requires case managers to ensure funded cases comply with the spirit of the Woolf reforms, in particular the overriding objectives of saving expense and dealing with the case in ways which are proportionate given the amount of money involved, the importance of the case and the complexity of the issues.”
It is stated at the outset of the Civil Procedure Rules that they have the “overriding objective of enabling the court to deal with cases justly.” Mr Justice Smith noted that the director made no mention in his statement of the other matters referred to in CPR 1.1(2) such as ensuring that the parties are on an equal footing (CPR
DISPUTE RESOLUTION
OCTOBER 2007
THE FETAL ANTI-CONVULSANT LITIGATION: WILL LSC FUNDING LIMITATIONS LEAD TO THE COLLAPSE OF YET ANOTHER PHARMACEUTICAL GROUP ACTION?
1.1(2)(a)), dealing with the case in ways which are proportionate to the financial position of each party (CPR 1.1(2)(c)(iv)), and ensuring that the case is dealt with expeditiously and fairly (CPR 1.1(2)(d)). According to the director’s statement, the LSC appeared to have elevated some of the various elements that the CPR identify as contributing to the overriding objective into distinct overriding objectives in their own right. Mr Justice Smith said he did not consider this to be helpful as the court has to seek to give effect to the overriding objective as a whole.
The director explained that following the decision in the judicial review proceedings, the LSC’s Funding Review Committee (“FRC”) concluded that the case “had sufficient merits to meet the merits test contained within the Funding Code as long as the case proceeded on the basis that the preliminary issue on defect, which was alone capable of derailing the litigation, was decided first…” If the case could not proceed by way of a trial on a preliminary issue then the case would be sent back to the FRC for review.
The Court’s Findings
The claimants therefore applied to have certain preliminary issues determined first. At the hearing, the claimants’ counsel expressed the opinion that unless the court acceded to the views of the LSC as to how this litigation should proceed, it was likely that funding would be discontinued. However, Mr Justice Smith thought this submission went further than the director’s evidence.
Assumptions
Mr Justice Smith firstly considered the assumptions upon which the claimants proposed that the preliminary issues be tried. He noted that particularly in complex cases, it was necessary that the assumptions be precise and unambiguous, as much of the purpose of having preliminary issues would be lost if the assumptions had to be expanded and explained by complicated scientific and pharmacological evidence.
His Honour found that the assumptions in the instant case did not, and however drafted could not, provide a clear and precise factual basis for the determination of the issues. For example, one of the claimants’ assumptions was that Epilim “is unsafe for all pregnant women whose fetuses are exposed to it.” Yet, it was unclear what the description of “unsafe” meant. Nor was it clear what was the degree of risk and what potential damage and/or disabilities would be sufficient for the drug to be described this way. Whilst he accepted that it may be necessary to supplement assumptions with some limited evidence, the more that is required, the less attractive the proposal for preliminary issues becomes.
Preliminary Issues
Mr Justice Smith then considered the preliminary issues that the claimants proposed and found these to also be problematic. For example, one of the issues assumed there had been an "occurrence" when this was still in dispute. Another issue could not be satisfactorily decided without a firm factual and evidential basis. Mr Justice Smith therefore rejected the claimants’ application for an order for the trial of the questions as preliminary issues.
Comment
It remains to be seen whether the LSC will now pull the plug on the funding of the FAC litigation - an outcome that the claimants' counsel clearly thought was likely. Without public funding, this litigation will inevitably become the latest in a long list of group actions doomed to failure in recent years. The LSC currently funds major group actions out of a budget of £3m per annum, which potentially limits the scope of major new group litigation. Funding for group actions is under far greater control than ever before through the LSC’s Special Cases Unit and in a recent article Colin Stutt, the Head of Funding Policy at the LSC, noted that pharmaceutical actions remain “very problematic”2.
However, there may be some light at the end of the tunnel for claimants hoping to pursue pharmaceutical group actions in the future. In June this year a series of recommendations were made by the Civil Justice Council to the Lord Chancellor to improve access to justice through the development of improved funding structures.3 One of the recommendations was for the introduction of properly regulated contingency fees in multi party cases where no other form of funding is
2 C Stutt, “Who ate all the P.I.’s?” (2007) JPIL 81 at 82.
3 Civil Justice Council, “The Future Funding of Litigation – Alternative Funding Structures” June 2007. available. It may well be that contingency fees will become the mainstream funding alternative for pharmaceutical group actions in future, given the continued tightening of the LSC’s purse strings for such cases. However, the introduction of any such reforms is likely to come too late for the claimants in the FAC litigation.
If you would like any further information, please contact either of the following:
Simon Pearl
DDI: 020 7293 4041
E: spearl@dac.co.uk
Olya Melnitchouk
DDI: 020 7293 4506
E: omelnitchouk@dac.co.uk
This publication is not a substitute for detailed advice on specific transactions and problems and should not be taken as providing legal advice on any of the topics discussed.
name and company name.
http://www.dac.co.uk/documents/resources/newsletters/The_fetal_anti_convulsant_litigation_Dispute_Resolution_Wire
Thursday, 28 January 2010
Wednesday, 27 January 2010
Shelley Jofre SEROXAT… we decided to focus research into this drug
 2.30 in Jofre says - ” read a little bit in news paper about patients complaints” year 2000 about ” Seroxat difficult to withdraw from” .. Jofre found it intriguing Jofre had only just started working on Panorama at that stage
2.30 in Jofre says - ” read a little bit in news paper about patients complaints” year 2000 about ” Seroxat difficult to withdraw from” .. Jofre found it intriguing Jofre had only just started working on Panorama at that stage3.30 in ” Jofre calls SSRI’s “SELECTIVE Serotonin Reuptake Inhibitors”
4.14 Jofre knew little of how the pharmcutical industry worked
4 .30 in Ed says - lets look at antidepressant story
4 45 Jofre says although problems with whole class of antidepressants we (bbc) decided to concentrate on Seroxat Why we narrowed down on Seroxat 1 because it was made by GSK 2 all the drugs in class cause suicidal thinking on dose change 3 Seroxat had a unique problem of withdrawal BECAUSE IT WAS LONGER ACTING … we decided to focus research into this drug
6.00 in - 40 min Panorama film took Shelley Jofre 8 months to make
6.10 in - It’s not something you do lightly WE WERE TAKING ON the worlds second largest drug company
7.30 We were talking to the lawyer the whole way through production
9.30 in - Jofre says “we took a punt” on Dr David Healy
Monday, 25 January 2010
Shelley Jofre who failed expectant mothers everywhere, she knew there was a problem with all SSRI, but only researched Seroxat to meet the requirements Seroxat lawyer Mark Harvey

Powered by Podbean.com
Shelley Jofre who failed expectant mothers everywhere, she knew there was a problem with all SSRI, but only researched Seroxat to meet the requirements Seroxat lawyer Mark Harvey
Jofre says although problems with whole class of antidepressants we (bbc) decided to concentrate on Seroxat Why we narrowed down on Seroxat 1 because it was made by GSK 2 all the drugs in class cause suicidal thinking on dose change 3 Seroxat had a unique problem of withdrawal BECAUSE IT WAS LONGER ACTING … we decided to focus research into this drug
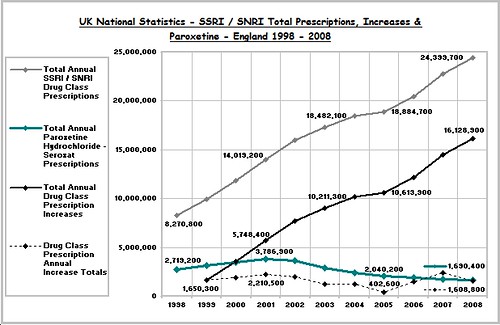
The Evidence, however is clear ... Seroxat decline UK

Chart 5 demonstrates the immense value to Society of free and independent Public ServiceBroadcasting and Internet communication. This combination has triggered the growth ofawareness of SSRI danger. It has united the many thousands of victims of SSRIs across theworld with some professionals who have laboured so long in a cause for saving lives, seekingjustice and exposing dysfunctional drug regulation. Chart 5 shows that the tide has turned inthe UK. Great encouragement should be taken from this life saving victory. However effortsmust continue both to expose the known risks of paroxetine (Seroxat, Paxil) and all the other illvalidated SSRIs and to call for the establishment an effective independent Drug SafetyRegulator in every country, the absence of which is the root cause of this ongoing officiallysupported tragedy
Saturday, 16 January 2010
Ironic !

Seroxat (Paroxetine).
The BMC are failing to recognise that he anti - depressant Seroxat is
addictive despite countless pleas from users that it is.
The BMC is made up of supposedly independant people - Ironic that nearly 3/4
of them have share in the Company, SmithGlaxoKlien - The Company that makes
Seroxat.
Bob
Birmingham
http://www.ds010a5436.pwp.blueyonder.co.uk/
---
Outgoing mail is certified Virus Free.
BOB 'THE CHAINSAW' FIDDAMAN
Checked by AVG anti-virus system (http://www.grisoft.com).
Version: 6.0.375 / Virus Database: 210 - Release Date: 10/07/2002
http://groups.google.com/group/uk.gov.social-security/browse_thread/thread/a14ee3fdb1191e86/44a8b0da27e6af87?hl=en&ie=UTF-8&q=seroxat
Friday, 15 January 2010

Thursday, 14 January 2010
The Evidence, however is clear ... Janice's husband John is presently taking Lustral NOT Seroxat !!

http://www.huntspost.co.uk/content/hunts/news/story.aspx?brand=HPTOnline&category=News&tBrand=cambs24&tCategory=NewsHPT&itemid=WEED07%20Feb%202007%2011%3A20%3A56%3A610
Tuesday, 12 January 2010
Seroxat User Group's Janice Simmons claims husband John "is one of worst affected" - "he's been taking Seroxat for 19 years" (but was she telling the truth?)
`Doctors are simply unaware of this withdrawal syndrome and unable to advise on what to do,' says Janice Simmons, co-ordinator of the Seroxat User Group.
Her husband John is one of the worst affected — she says each time he's tried to stop taking it, the symptoms have been so severe he's had to give up; he's been taking Seroxat for 19 years.
Read more: http://www.dailymail.co.uk/health/article-1242502/Hooked-happy-pills-Internal-bleeding-Strokes-Birth-defects-The-long-term-effects-antidepressants-terrifying.html#ixzz0cOocvmTH
Her husband John is one of the worst affected — she says each time he's tried to stop taking it, the symptoms have been so severe he's had to give up; he's been taking Seroxat for 19 years.
Read more: http://www.dailymail.co.uk/health/article-1242502/Hooked-happy-pills-Internal-bleeding-Strokes-Birth-defects-The-long-term-effects-antidepressants-terrifying.html#ixzz0cOocvmTH
Seroxt UK class action now only 500 clients says Daily Mail
extract
Around 500 people are suing GlaxoSmithKline on the grounds that the company concealed evidencethat their drug Seroxat (a selective serotonin re-uptake inhibitor) may cause withdrawal `syndrome' with symptoms including anxiety, pain, palpitations and memory lapses.
`Doctors are simply unaware of this withdrawal syndrome and unable to advise on what to do,' says Janice Simmons, co-ordinator of the Seroxat User Group.
Her husband John is one of the worst affected — she says each time he's tried to stop taking it, the symptoms have been so severe he's had to give up; he's been taking Seroxat for 19 years.
There are ways of tapering withdrawal - for instance, using a liquid dose of medication which can be gradually reduced far more easily than a tablet and which can normally be prescribed by GPs.
'The problem is most people haven't a clue how to access advice on withdrawal,' says David Healy, professor of psychological medicine at Cardiff University, whose protocol on the withdrawal of SSRIs is widely regarded as the best method of stopping the medication. 'GPs are rarely informed - and the pharmaceutical companies are unwilling to even admit that there is a problem.'
Read more: http://www.dailymail.co.uk/health/article-1242502/Hooked-happy-pills-Internal-bleeding-Strokes-Birth-defects-The-long-term-effects-antidepressants-terrifying.html#ixzz0cOocvmTH
Around 500 people are suing GlaxoSmithKline on the grounds that the company concealed evidencethat their drug Seroxat (a selective serotonin re-uptake inhibitor) may cause withdrawal `syndrome' with symptoms including anxiety, pain, palpitations and memory lapses.
`Doctors are simply unaware of this withdrawal syndrome and unable to advise on what to do,' says Janice Simmons, co-ordinator of the Seroxat User Group.
Her husband John is one of the worst affected — she says each time he's tried to stop taking it, the symptoms have been so severe he's had to give up; he's been taking Seroxat for 19 years.
There are ways of tapering withdrawal - for instance, using a liquid dose of medication which can be gradually reduced far more easily than a tablet and which can normally be prescribed by GPs.
'The problem is most people haven't a clue how to access advice on withdrawal,' says David Healy, professor of psychological medicine at Cardiff University, whose protocol on the withdrawal of SSRIs is widely regarded as the best method of stopping the medication. 'GPs are rarely informed - and the pharmaceutical companies are unwilling to even admit that there is a problem.'
Read more: http://www.dailymail.co.uk/health/article-1242502/Hooked-happy-pills-Internal-bleeding-Strokes-Birth-defects-The-long-term-effects-antidepressants-terrifying.html#ixzz0cOocvmTH
Monday, 11 January 2010


Friday, 8 January 2010
it's 2010 & Seroxat Group Litigation Order is going to be tested - so what are the ISSUES?

http://www.hmcourts-service.gov.uk/cms/150_14671.htm
Name of Group Litigation Order: Seroxat Group Litigation
Lead Solicitors: Hugh James Solicitors (Harmful Products Department) of Hodge House, 114-116 St Mary Street, Cardiff CF10 1DY
Defining Issues:
Defining Issues:-Does Seroxat have a capacity to cause asverse effects consequent upon or following discontinuance (withdrawl) such as prevent or make more difficult the ability of users to discontinue, withdraw from or remain free from taking Seroxat to a greater extent than all other Selective Serotonin Re-uptake Inhibitors (SSRIs)
Seroxat

Court sets deadline for compensation claims.
Have you had difficulties withdrawing from the anti-depressant drug Seroxat?
Have you found it impossible to withdraw from it? Are you having difficulties in withdrawing from Seroxat now?
The High Court made a Group Litigation Order in relation to the Group Action brought by around 500 individuals alleging harm from problems withdrawing from Seroxat.
On 19 May 2009 the High Court ordered that any individual who wishes to pursue a compensation claim must join the Group Action before 15 January 2010.
All individuals must have their claim investigated before they can join the action and so they need to come forward ASAP.
Register your interest now, call the Seroxat team at Hugh James, designated as lead solicitors for the purposes of the Group Litigation Order, on 02920 785 971 or go to www.hughjames.com/seroxat
The Group Register will close on 15 January 2010 and any individuals who have not joined at that date may lose their opportunity to be part of the litigation.
You should not stop taking any medication without consulting your doctor
Tuesday, 5 January 2010
BBSRC check out the original & best BobFiddaman blog
Host Name arcl11.cc.bbsrc.ac.uk
IP Address 149.155.96.6
ISP BIOTECHNOLOGY AND BIOLOGICAL SCIENCE RESEARCH COUNCIL
Domain BBSRC.AC.UK
City CAMBRIDGE
Region ENGLAND
Country UNITED KINGDOM
Date Time WebPages
January 05, 2010 2:18:57 PM SEROXAT SUFFERERS - STAND UP AND BE COUNTED
http://bobfiddaman.blogspot.com/
http://www.google.co.uk/search?q=%22bob%20fiddaman%22&hl=en&ie=UTF-8&tab=nw
IP Address 149.155.96.6
ISP BIOTECHNOLOGY AND BIOLOGICAL SCIENCE RESEARCH COUNCIL
Domain BBSRC.AC.UK
City CAMBRIDGE
Region ENGLAND
Country UNITED KINGDOM
Date Time WebPages
January 05, 2010 2:18:57 PM SEROXAT SUFFERERS - STAND UP AND BE COUNTED
http://bobfiddaman.blogspot.com/
http://www.google.co.uk/search?q=%22bob%20fiddaman%22&hl=en&ie=UTF-8&tab=nw
Sunday, 3 January 2010
Chapter 3 is factually inaccurate - Fiddaman weakened his own case says Phatmacologist
The purpose of my original post was just to point out that chapter 3 is factually inaccurate. I've no objection to somebody putting the case against GSK's marketing of paroxetine into a first-person narrative. However, the case is weakened if it's based in part on demonstrably incorrect arguments about the pathology and pharmacology of depression.
http://www.authonomy.com/ViewBook.aspx?bookid=15084
http://www.authonomy.com/ViewBook.aspx?bookid=15084
Saturday, 2 January 2010
Fiddaman's drug cocktail called "risky" by professional pharmacologist
View Book:
"However, giving two anti-depressants plus tramadol simultaneously sounds risky. Where is it stated that the author was taking these drugs in combination? I've only read chapters 1 and 3."
"However, giving two anti-depressants plus tramadol simultaneously sounds risky. Where is it stated that the author was taking these drugs in combination? I've only read chapters 1 and 3."
- http://www.authonomy.com/ViewBook.aspx?bookid=15084
Subscribe to:
Posts (Atom)